GAO Report Recommends That CMS Expand Hospice Abuse Reporting Requirements
| Footnotes for this article are available at the end of this page. |
The US Government Accountability Office (“GAO”) issued a report on December 12, 2022, recommending that the Centers for Medicare and Medicaid Services (“CMS”) expand hospice abuse and neglect reporting requirements to make them more akin to nursing homes and hospitals. This would require hospice care providers to report all instances of suspected abuse and neglect immediately — even those instances involving suspected perpetrators unaffiliated with the hospice care providers, like family members. The Department of Health and Human Services (“HHS”) neither agreed nor disagreed with GAO’s recommendation.
Current Hospice Policy Compared to Nursing Home and Hospital Policy
Under current policy, hospice care providers are required to report allegations of abuse or neglect to the appropriate state authorities: (1) if the alleged perpetrator is affiliated with the hospice; and (2) after the hospice has verified it as abuse or neglect based on an internal investigation, which may take up to five days. 42 C.F.R. § 418.52(b).
Under the first requirement, hospice providers currently have no obligation to report suspected abuse or neglect by any unaffiliated third party. This is important because studies indicate that most abuse in the hospice setting occurs in the home by individual caregivers, such as family members, not by the hospice care provider or its affiliates.1 Therefore, in most instances, there is no requirement to report suspected abuse. In the hospital and nursing home settings, providers are required to report any suspected abuse or neglect regardless of who is involved. 42 C.F.R. § 483.12(c)(1).
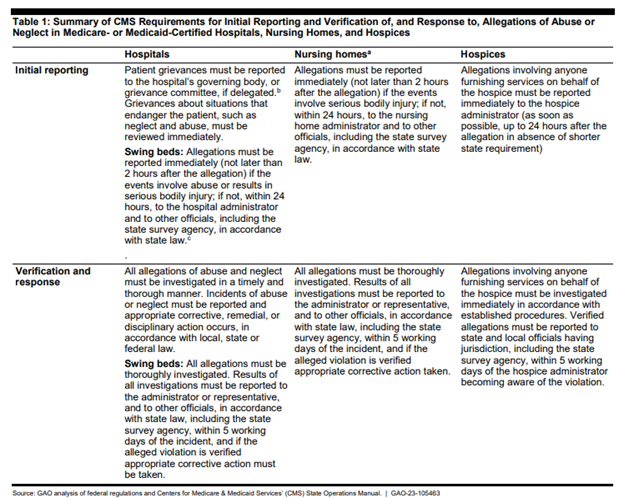
Under the second requirement of the current policy, reporting only occurs after an internal investigation by the hospice care provider. In nursing homes and hospitals, reporting must occur immediately after the suspected abuse is recognized. 42 C.F.R. § 483.12(c)(1). This chart from the GAO Report compares the current reporting obligations among the three provider types. Specifically, nursing homes and hospitals must report all instances of suspected abuse or neglect resulting in serious bodily harm within two hours and in all other instances within 24 hours. 42 C.F.R. § 483.12(c)(1). This allows CMS to quickly initiate unannounced on-site investigations of its own to confirm that providers are conducting thorough investigations and adequately protecting their patients, even while not under their care.
GAO’s Recommendation and Potential Implications
GAO recommended that CMS require hospice care providers to immediately report all instances of suspected abuse or neglect to the appropriate survey agencies irrespective of the perpetrator. This places a heavy burden on hospice care providers who could potentially face survey enforcement actions for issues that fall within a gray zone of abuse and neglect. Unlike other provider types, hospice staff have infrequent interactions with patients and family, often as little as two times per week for the most common form of hospice — routine care. Moreover, hospice patients are, by definition, in a terminal decline, with frequent instances of unpreventable skin breakdown, significant weight losss, infections, falls, and incontinence. With falls and wasting of muscle and fat reserves comes increased bruising and easier skin tears. Thus, what in an institutional setting may appear, at first blush, to be potential neglect or abuse could be representative of the terminal decline for many hospice patients living at home. Likewise, when issues are observed contemporaneously and continuously in an institutional setting, such as a fall with resulting bruising developing over a few days, the same injuries observed only intermittently in a home setting may appear more alarming.
Therefore, to engraft an institutional reporting system onto hospice providers could lead to over-reporting of suspected abuse and neglect issues. It also places a more significant wedge between caregivers and family members, where the providers are entering the home only periodically and again not observing issues contemporaneously. And then, of course, there is the lack of adequate survey staff to investigate allegations. To call upon surveyors to understand the nuances of the hospice terminal decline and the expected body system breakdowns that accompany that decline and then distinguish that from abuse and neglect could be asking too much. To place hospices in a position of potential survey enforcement for failure to report and being second-guessed where potential signs of abuse and neglect are equally consistent with a normal and expected terminal decline could be going too far, especially when the hospice staff observing these signs may have only intermittent interactions with patients and families. Notwithstanding these challenges, the industry should carefully consider whether to oppose any new proposals flowing from the GAO Report, as the optics could be less than ideal if not handled delicately.
[1] Study cited by GAO: Department of Health and Human Services Office of Inspector General, CMS Could Use Medicare Data To Identify Instances of Potential Abuse or Neglect, A-01-17-00513 (Washington, D.C.: June 2019); 7K. M. Jayawardena and S. Liao, “Elder Abuse at End of Life,” Journal of Palliative Medicine, vol. 9, no. 1 (2006): 127.
Related Services
Related Industries
- Jason E. Bring
Partner

{kind=link}